The ideal systolic blood pressure (SBP) target has been a matter of investigation for years, particularly in elderly patients. The Systolic Blood pressure Intervention Trial (SPRINT) final results have now been published and reveal a lower all-cause mortality and major adverse cardiovascular event rate (MACE) with an intensive control strategy (SBP <120 mmHg) when compared to standard target (SBP<140 mmHg) in hypertensive patients without diabetes or previous stoke.1
Prior studies (ACCORD BP, SPSS3-BP) have shown no benefit in intensive vs. standard SBP control in patients with diabetes or previous stroke. The SPRINT-trial addressed the ideal SBP target for patients without prior stroke, diabetes, or dementia. It enrolled patients with age >50 years (mean age, 68 years) and at least one cardiovascular risk factor and randomized in 1:1 fashion to intensive vs. standard care therapy. A specific algorithm was followed to achieve target SBP.
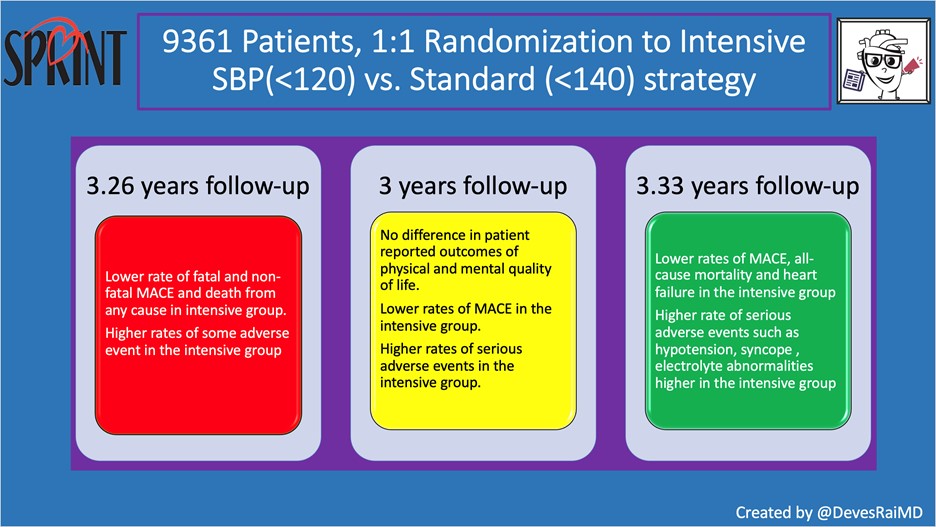
Figure. SPRINT Design and Results. Credit: Devesh Rai, MD
Enrollment stopped early at median follow-up of 3.26 years owing to significant cardiovascular benefits seen in the intensive control arm with a lower rate of MACE and all-cause mortality.2 Patient-reported outcomes were similar in both groups (see Figure).3
After the trial was stopped early, patients returned to their usual health care providers for further management in the postintervention observational period. At a median follow-up of 3.33 years, the primary outcome and all-cause mortality remained significantly lower in the intensive control group during receipt of the randomly assigned therapy and after the trial (see Figure). However, the intensive control group had more serious adverse events (hypotension, syncope, AKI, and electrolyte abnormalities).1 The magnitude and pattern of differences in adverse events according to treatment assignment among participants >75 years of age were similar to those in the overall cohort. 1
Based on the SPRINT trial, many guidelines now recommend that certain high-risk patients with high blood pressure aim for a systolic blood pressure below 130 rather than the standard target of 140. (SPRINT aimed for <120/80.) 7/ pic.twitter.com/HVbhjzuSjs
— Dr. Tom Frieden (@DrTomFrieden) May 21, 2021
Dr. Oscar Cingolani, Director of the Hypertension Center at the Johns Hopkins Hospital said the following: “The fact that more patients treated to a more aggressive target had more adverse events, brings “quality of life” factor to table. Imagine two different scenarios. The patient who can be easily brought to a target of 120/80 with 2-3 medications, versus the patient requiring multiple medications. The latter are those who tend to have problems with side-effects. Thus, treatment should still be personalized.”
While current guidelines advise target of <140/90 mm Hg for blood pressure control,4 the strong mortality benefits and reduction of MACE seen in SPRINT are likely to impact clinical practice guidelines for non-diabetic patients with hypertension and increased cardiovascular risk, including elderly patients.
References
- Final Report of a Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2021;384(20):1921-1930.
- A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2015;373(22):2103-2116.
- Berlowitz DR, Foy CG, Kazis LE, et al. Effect of Intensive Blood-Pressure Treatment on Patient-Reported Outcomes. N Engl J Med. 2017;377(8):733-744.
- Unger T, Borghi C, Charchar F, et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension. 2020;75(6):1334-1357.
Credit: Original article published here.